Food addiction or Eating Disorder: The Unified Theory of Restrictive and Addictive Eating
 Vanessa Kredler
Vanessa Kredler 
Discover the relationship between food addiction, eating disorders, generational trauma, and neurodivergence.
Key Summary
This blog explores how a groundbreaking 2026 theoretical review by Dr. David A. Wiss and Alan C. Logan completely dismantles the polarising clinical "civil war" between traditional eating disorder frameworks and the food addiction model. By introducing a unified life course model, the authors prove that restrictive eating and ultra-processed food use disorder (UPFUD) are not separate, rigid diagnostic boxes, but are rather fluid survival trajectories sharing the exact same biological roots: generational trauma, adverse childhood experiences, and heritable neurodiversity. This landmark paper provides the definitive, trauma-informed framework we need to deliver truly person-centred, precision recovery.
Food addiction and eating disorder polarisations
For decades, a rigid ideological civil war has fractured the eating pathology landscape. On one side stands traditional eating disorder (ED) treatment, operating primarily on the foundational premise that all binge eating or loss-of-control consumption is a direct, homeostatic reaction to dietary restriction. On the other side sits the food addiction model, arguing that specific neurochemical profiles interact with modern ultra-processed food environments to produce genuine substance-like dependency. There are also ongoing discussions about how food addiction is different from binge eating disorder.
Lived and Clinical Experience: Why This Study Lights Me Up
From my lived experience, and working directly in clinical practice, things are never clear cut in reality. I routinely work with clients who present with clear addictive histories and who self-identify as addicted, yet traditional clinical pathways to treat eating disorders demand we tell them "all foods fit”. Insistence on this formulaic treatment model has left clients struggling with compulsive eating, binge eating disorder, and chronic relapse feeling misunderstood, misdiagnosed, and deeply ashamed. Clients have reported feeling more out of control in their eating after having been treated for binge eating disorder and trying diligently to eat all foods in moderation. It just didn’t work for them.
A groundbreaking theoretical review published in the Journal of Eating Disorders (2026) by Dr. David A. Wiss and Alan C. Logan has shattered this dichotomy. Their paper, "A unified theory of restrictive and addictive eating: a life course model integrating generational transmission, neurodevelopmental risk, and ultra-processed food use disorder," provides the missing clinical link. It validates exactly what I observe daily in my practice: eating patterns exist on a fluid, biological, and trauma-informed continuum.
It’s rare that someone presents with food addiction where it’s only about the specific foods (though it does happen). Most of the time, we are dealing with a messy cluster of compulsive eating, partly to chase an addictive high, and partly to satisfy insatiable cravings, and partly because of an uncontrollable experience of “I just can’t stop eating”. This often goes along with other addictive and compulsive behaviours, be they use of other substances such as alcohol and drugs (past or present), or behaviours such as over-working, excessive Internet use or the “over or under-doing” of any activity, which becomes compulsive, distressing and harmful.
On top of that, in my experience there is a high overlap with neurodivergence, to the point that the addictive/compulsive patterns inherently feel so wired in to the person that they feel like neurodivergence even without a diagnosis of ADHD or similar diagnosis being present. Upon deeper exploration there is almost always intergenerational trauma, particularly attachment injury, in my clients.
That’s why I lit up when I read the article, which confirms my deepest knowing of what is true, despite where the evidence is at present. That’s the power of lived experience. No scientist can take your experience away from you.
The Shared Roots: Generational Trauma and ACEs
The core genius of the Wiss and Logan model is its foundation. Rather than starting at the onset of dietary restriction or the first exposure to highly palatable foods, the model traces eating pathology back to its origin: generational transmission and Adverse Childhood Experiences (ACEs).
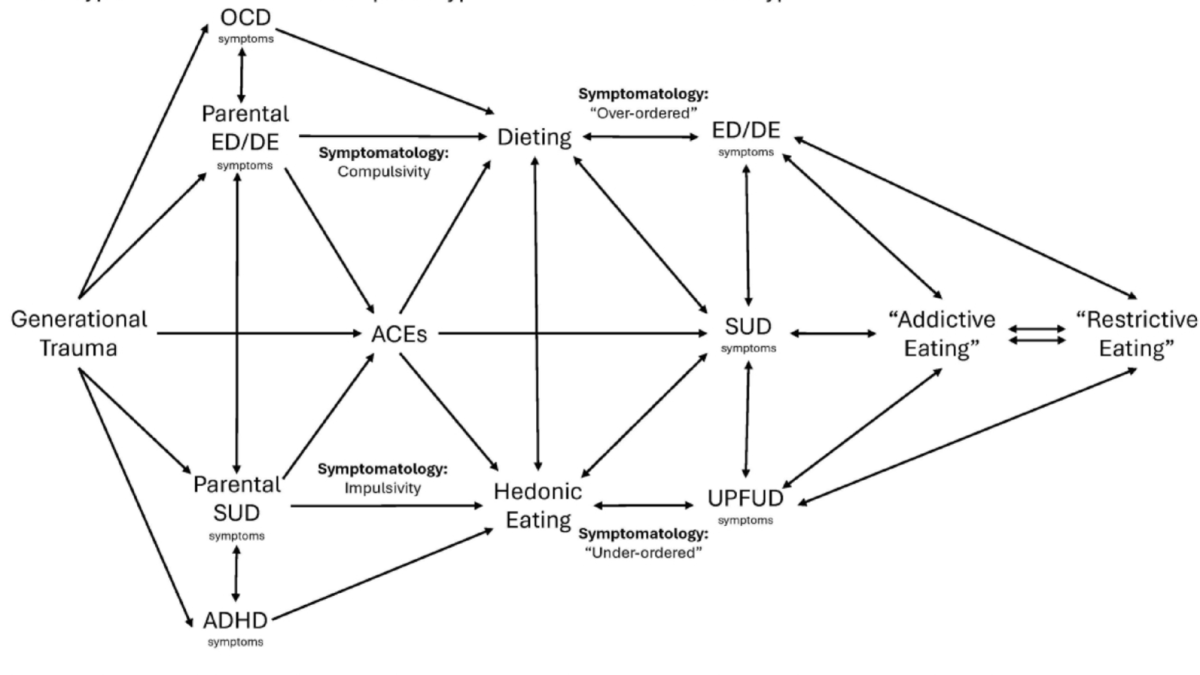
The authors demonstrate that early developmental trauma alters the hypothalamic-pituitary-adrenal (HPA) axis and shifts the nervous system into a perpetual state of survival. When a child grows up facing chronic stress, neglect, or relational trauma, their biology adapts. From this shared soil of trauma, the model identifies two distinct, divergent neurodevelopmental legacy pathways that dictate how an individual will later relate to food. These pathways are shown in the image above, reproduced here with permission from the authors):
Pathway 1: The Restrictive Eating Trajectory (The OCD Phenotype): This pathway typically manifests in families with strong expressions of obsessive-compulsive traits, rigid behavioural boundaries, or extreme perfectionism. In this context, developmental trauma manifests as an intense need for environmental and somatic control. Food restriction, calorie counting, and body manipulation become maladaptive survival strategies to regulate an overwhelmed nervous system.
Pathway 2: The Addictive Eating Trajectory (The ADHD/SUD Phenotype): Conversely, this trajectory branches from families with a high heritability of impulsive traits, Attention-Deficit/Hyperactivity Disorder (ADHD), or Substance Use Disorders (SUDs). When developmental trauma hits this specific neurobiological profile, it blunts the dopamine reward pathways. The individual doesn't look for rigid control; they look for chemical regulation. This opens the gate directly to Ultra-Processed Food Use Disorder (UPFUD)—using chemically engineered foods to self-medicate an under-stimulated, traumatised nervous system.
The Biological Reality of "Symptom Substitution"
One of the most profound validations this paper offers to my clinical practice is its exploration of cross-addiction and sobriety. Many of my Australian clients arrive in my clinic after successfully navigating recovery from alcohol or drug dependency, only to find themselves completely blindsided by a sudden, fierce addiction to ultra-processed foods. Equally, they may get on top of their food addiction and realise they have been over-working.
Traditional frameworks dismiss this as merely "swapping vices" or state that it's a natural phase of early recovery. Wiss and Logan prove it is deeply biological. When an individual achieves sobriety from an external substance, the underlying traumatised neurobiology and its craving for dopaminergic reward remains unchanged. Without targeted, food-specific addiction treatment, the brain naturally pivots to the most accessible, socially acceptable reward available: engineered hyper-palatable foods. It is not a lack of willpower; it is a predictable biological trajectory. That’s why many people who seek bariatric surgery end up becoming addicted to alcohol.
Fluidity and Crossover: Breaking the Clinical Boxes
Crucially, this model rejects the idea that the individual belongs permanently in a single diagnostic box. The authors emphasise that individuals frequently experience both pathways simultaneously or cross over from one to another across their lifespan.
For example, a person may start on the restrictive pathway, utilising food avoidance to gain a sense of control over childhood trauma. However, chronic caloric deprivation combined with exposure to modern food environments can trigger a profound shift in reward processing, moving them down the addictive eating pathway into severe binge patterns. Understanding this fluidity allows us to build dynamic, evolutionary treatment protocols rather than forcing a client into a rigid category that doesn't fit their lived reality.
A New Era of Precision Treatment
The implications of this paper for the future of nutritional psychology, metabolic psychiatry, and food addiction treatment are monumental. It demands that we move past one-size-fits-all treatments and become what trauma-informed therapists have always been good at: to be truly person-centred.
This framework forms the backbone of how we should assess and treat food dependency. By mapping an individual’s familial heritability, trauma markers and history with addictive and restrictive eating, as well as other compulsive behaviours and mental health challenges. My experience is that we can co-create a recovery plan that actually respects their living experience.
If you have spent years feeling like your struggle with food is a personal moral failure, let this scientific breakthrough be your reassurance: it is biology, it is history, and it is treatable and it’s your unique journey but…you don’t do it alone. Contact me to get help.
Categories: : Eating Disorders, Food Addiction, Trauma

Acknowledgement of Country
I recognise the history, culture, diversity and value of all Aboriginal and Torres Strait Islanders, and acknowledge their Elders past and present.
I acknowledge that sovereignty has never been ceded, and support reconciliation, justice and the recognition of the ongoing living culture of all First Nations people by providing welcoming and culturally informed services.
Embracing inclusivity and diversity, I also support a culture of inclusion, respect, choice, voice and diversity and am committed to supporting all people to be mentally well and engaged in their communities.
